

What We Have Left Undone


Let justice roll down like waters.
Amos 5:24
Dear Friends and Colleagues,
The prayer of confession in the Book of Common Prayer contains the familiar phrase, “what we have done and what we have left undone.”
In many religious traditions, there is the concept of sins of “commission”, the wrongs that we do, and also “omission”, what we fail to do. We aren’t just held responsible for a bad action but also the failure to do good, support justice or defend the vulnerable. The Hebrew prophets make this especially clear that those who are in power are held to account for their failure to help those in need.
A new report from the Cato Institute takes an important look at our current overdose crisis. Instead of telling a story that reduces the opioid epidemic to the actions of Big Pharma and overprescribing doctors they detail the history of law enforcement and the federal government restricting the ability of doctors to practice medicine. Sometimes the greater danger lies in when doctors are unable to prescribe as they should more than when they prescribe when they shouldn’t.
In theological terms, they tell the story of the sins of omission and what has been “left undone” often at the behest of powerful interests restricting the medical judgment of doctors.
When I have told the story of my own hospitalization and subsequent development of an opioid use disorder, I’ve often had others respond with an immediate condemnation of the doctors who prescribed me opioids.
I have had to repeat over and over again: the doctors did nothing wrong by prescribing me opioids. They were medically necessary and appropriate.
Even once I developed an opioid use disorder the greatest threat to my life and health was not my prescription to opioids. What would have been most dangerous, and I was lucky to avoid, would have been a rapid taper or immediate stop to my prescription. This could have led me to seek far more dangerous and unregulated alternatives from an illicit market as so many others have felt forced to do.
The reality was that I was simultaneously addicted and still in severe pain that required pain medication. My doctor understood this and continued to allow me access to prescription opioids while I received treatment through cognitive behavioral therapy and began experimenting with alternative pain management therapies as we found what worked for me.
What would have harmed me the most was not a sin of commission (the prescription) but one of omission, failing to provide needed pain medicine from a safe and reliable source.
As the Cato report details, many doctors today live under fear that if they exercise their best medical judgment, they may become a target of law enforcement. As a result, doctors are abandoning pain patients, living under the threat of law enforcement or even being arrested for practicing medicine. Pain patients are losing access to the medications they need and are turning to a dangerous illicit supply or even dying by suicide.
Our roundup today gives you highlights from the new Cato report as well as work from journalist Maia Szalavitz about the harsh consequences of these systemic failures.
Yes, it is important that opioids are prescribed responsibly. Yes, doctors should be held responsible to medical boards if they fail to practice medicine to the highest standards. Yes, law enforcement has a role if they discover actual “pill mills.”
But we also need to talk about the sins of commission when politics gets in the way of doctors practicing responsible medicine or law enforcement starts dictating standards of public health.
It’s not just about what is done, but what is left undone.
Keep the faith,
Timothy McMahan King
Senior Fellow, Clergy for a New Drug Policy
The War on Drugs has greatly impacted the practice of medicine. In particular, pain patients have been harmed as policymakers pressure doctors to taper or discontinue prescribing opioids.
A recent study by the CATO Institute analyzed how the government and law enforcement increasingly surveil and influence the way doctors treat pain, psychoactive substance use, and substance use disorder.
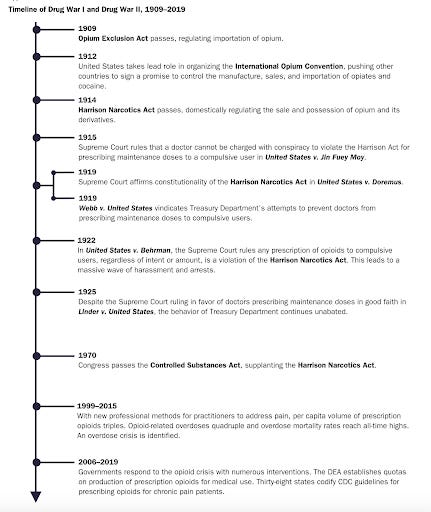
Authors Jeffrey A. Singer and Trevor Burrus explore how two discernible waves, Drug War I and Drug War II have destructively intruded on the patient-doctor relationship. The authors argue that both waves were shaped by law and society’s view of people who use opioids and cocaine as immoral.
Research and roundup compiled by Cassidy Willard, Research Associate

Image source: www.cato.org
Although it seems surprising to many of us, opium and its derivatives were broadly legal in the United States before 1914.
“The image of the opioid user was entirely different in the late 19th century from today. Doctors prescribed opium for many ailments because it often helped.”
In fact, opium was often prescribed as a cough suppressant, and to alleviate pain, soothe nerves, and calm anxieties.
Additionally, “opioid users of the time were usually regarded as less morally reprehensible than those who habitually consumed “demon rum” in saloons, burning through their paychecks night after night and leaving their families destitute. Opium users with a reliable supply could be, and often were, upstanding members of society. As long as they could maintain a supply, opioid addiction did not necessarily entail almost any of the imagery we associate with users today: gaunt, pale, sickly “junkies” willing to do anything to get the next fix.”
This view of opioids began to change with the federal Harrison Narcotics Act.
“The Harrison Act was the first significant federal drug law in the United States and, as amended, was the basic federal drug law for 56 years until the Controlled Substances Act was passed in 1970. There were earlier laws, such as the Opium Exclusion Act of 1909 that regulated the importation of opium, but the Harrison Act was the first to domestically regulate the sale and possession of opium and its derivatives.”
The interpretation and enforcement of the Harrison Narcotics Act created new problems for physicians. The statute did not define key terms like the requirement to “personally attend” to patients, or “professional practice” and “good faith.”
The Harrison Act finally reached the Supreme Court in December 1915. The court took numerous challenges of the statute but “was careful to choose those cases in which the doctor’s behavior was egregious.” In 1922, the Supreme Court decided United States v. Behrman. Ruling “against the doctor, the six justices decided that not only would they read substantive medical standards into the statute—defining “professional practice” when the statute intentionally did not—but they would enforce their own views, rather than medical experts’ views, as to what constitutes acceptable medical practices.”
This ruling unleashed what drug‐war historian Rufus King deemed “a reign of terror.”
“Treasury agents began ‘threatening doctors who had anything further to do with drug addicts, and sending a goodly number of recalcitrant practitioners off to prison with the Behrman formula…the addict‐patient vanished; the addict criminal emerged in his place.’ Whereas Treasury agents had initially been charged by the Harrison Act with policing professions that provided opioids and keeping the trade visible and above ground, they now were hounding everyone and throwing thousands of people in jail, while the market for opioids began moving underground.”
Although a later decision in Linder v. United States vindicated a doctor who prescribed maintenance doses in good faith, “the government essentially pretended that the Linder decision didn’t exist.”
The treasury department had essentially unfettered power to regulate, police, and prosecute doctors prescribing opioids.
Today, the cycle continues. Doctor-patient relationships are again being dictated by federal law enforcement and policed by government agencies.
Today, the cycle continues. Doctor-patient relationships are again being dictated by federal law enforcement and policed by government agencies.
Substance use is a health issue and must be viewed as one. Law enforcement and government officials are not trained in pain management. “The management of acute and chronic pain involves the same nuanced medical decision-making as does the treatment of hypertension, diabetes, infectious diseases, and psychiatric disorders.”
“Although the reduction in opioid prescriptions has had no impact on the overdose deaths from medically used opioids, the same cannot be said for opioids as a whole. It is now widely accepted that as the supply of relatively safe prescription drugs was slashed, both users and abusers have turned to heroin and, more recently, fentanyl, which is responsible for 87% of the 30,000 spike in drug overdose deaths in 2020.”
Yet, “policymakers refuse to reassess their assumption that the overdose crisis was caused by doctors overprescribing opioids.”
“The study also provides empiric evidence of what health‐care providers have been seeing ever since policymakers began pressuring them to taper or discontinue prescribing opioids to their patients in pain: tapering the opioids that were controlling their pain was associated with a 68% increase in overdoses and doubling of mental health crises, which can be subdivided into depression (up 346%), anxiety (up 79%), and suicide attempts (up 430%).”
The question then becomes “How can we possibly even consider, let alone implement, policies that result in such damage?
According to author Maia Szalavitz pain patients that genuinely need painkilling drugs are now subject to random reports to the doctor's office for pill counts, prescription limits, extra refill appointments, urine testing, and other restrictions.
Although the classic government line is that the opioid epidemic is linked to increased use of pain medications being prescribed; however, “the overwhelming majority of addictions do not start with a prescription—and most opioid prescriptions do not cause addiction. Instead, opioid addiction usually begins in the same place that all other addictions start: in the childhoods, traumas, mental illnesses, and genes of those affected.”
Pain patients are suffering because the government refuses to acknowledge their missteps.
“Mistreating patients doesn't stop addiction; that requires compassionate care.”